
Urine tests can help find out if you have a urinary tract infection (UTI). Urinalysis and urine culture (MC/S) look for the bacteria that cause infection and sensitivity testing can show which antibiotics are likely to be effective in treating the infection. UTIs affect the bladder and/or the kidneys. Bladder infections are more common and are known as uncomplicated UTIs or cystitis. They occur when bacteria get into the urethra – the tube through which the urine leaves the body – and travel up into the bladder. A complicated UTI is when the infection travels beyond the bladder up to the kidneys.
What is it?
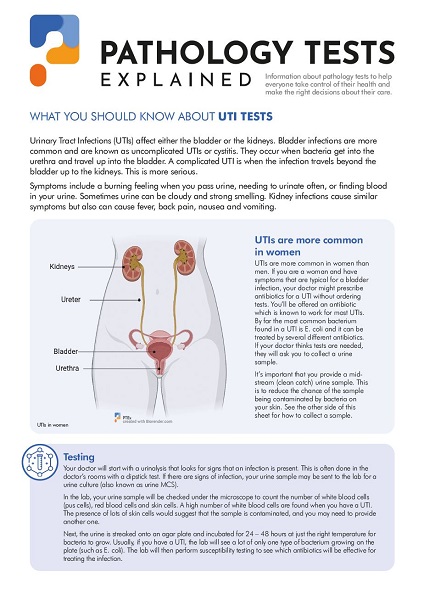
A UTI is an infection of one or more parts of the urinary tract. The urinary tract consists of two kidneys, two ureters, a bladder, and a urethra. The kidneys are bean-shaped organs found in the lower back below the ribcage. They filter waste out of the blood and produce urine to carry the waste and excess water out of the body. The urine is carried through the ureters (tubes) from the kidneys to the bladder.
The bladder is a hollow muscular organ that stores urine for a short time period. The bladder stretches as urine accumulates and at a certain point it signals to the body that it needs to relieve the growing pressure. A muscular valve (sphincter) at the opening of the bladder is relaxed and the bladder contracts to send urine through the urethra (a tube linking the bladder to the external surface of a persons skin) and out of the body.
A UTI can be due to infection in any part of the urinary tract. The most common type is infection involving the bladder (also known as cystitis). If the infection then spreads to the kidneys it is called pyelonephritis.
Common causes
Urine does not normally contain microorganisms, but if urine is obstructed from leaving the body or retained in the bladder, it provides a good environment for bacteria to grow. Most urinary tract infections are due to bacteria that are introduced into the opening of the urethra. They stick to the walls of the urethra, multiplying and moving up the urethra to the bladder.
Most UTIs remain in the lower urinary tract (urethra or bladder) where they cause annoying symptoms, such as a burning sensation during urination, but are more easily treated. While these infections are easily treated in most cases, if inadequately treated, the infection may spread up through the ureters, and into the kidneys which is a more serious condition which in rare cases can cause permanent kidney damage and needs a longer course of antibiotics. In some cases a urinary tract infection may lead to an infection in the bloodstream (septicaemia) that can be life-threatening.
Although a variety of bacteria can cause UTIs, most (80 to 90 percent) are due to Escherichia coli, a bacterium that is common in the gastrointestinal tract and is routinely found in stool (faeces). Other bacteria that may cause UTIs include species of: Proteus, Klebsiella, Enterococcus and Staphylococcus. Occasionally, a UTI may be due to a yeast, such as Candida albicans. Urethritis (infection involving the urethra) is often due to a sexually transmitted disease such as herpes, chlamydia, or gonorrhoea.
Although anyone at any age can have a UTI, women are much more likely than men to have them. It is thought that this is partly anatomical, because a woman’s urethra is shorter (less distance for bacteria to travel) and because their anus and vagina are relatively close to the urethra. Anything that slows down the passage of the urine, blocks it, or introduces bacteria into the urinary tract can raise a patient’s risk of having a UTI.
Conditions that cause an increased risk for developing a UTI include:
Signs and symptoms
Although UTI symptoms vary, many people will experience:
Complications
In most cases, UTIs are acute and uncomplicated. They are treated and the symptoms subside within a day or two. UTIs that spread to the kidneys, however, may cause permanent kidney damage, especially in children and the elderly if the infections are recurrent.
In some circumstances, urinary infections and sepsis (infection of the blood) can be life-threatening conditions requiring hospitalisation and immediate treatment.
In pregnant women, a UTI can lead to premature labour and delivery and cause high blood pressure. In men, a UTI can cause prostate infection and inflammation, which can be difficult to treat.
Tests
Common Laboratory Tests
Most UTIs are detected by performing a urinalysis and then confirmed with a urine culture. If there are pathogenic (disease-causing) bacteria present, then susceptibility testing is done to make sure that the antibiotic that the doctor chooses will effectively treat the microorganism causing the infection.
Follow-up Laboratory Tests
If a doctor suspects that a UTI may have spread into the bloodstream, a blood culture may be ordered. If symptoms are suspected to be due to a sexually transmitted infection (STI), such as chlamydia or gonorrhoea, then specific tests for STIs will be ordered on the urine sample.
In the case of recurrent or chronic urinary tract infections, other laboratory tests such as glucose (to check for diabetes) or urea and creatinine (to evaluate kidney function) may also be done.
Non-Laboratory Tests
Imaging scans and special X-rays may also be used to look structural or functional problems and/or signs of an underlying disease or condition. If a person has recurrent or chronic UTIs, one or more of the following procedures may be ordered. Each gives the doctor different information.
Prevention and treatment
Prevention of a UTI centres on keeping the urine moving through the urinary tract and avoiding bacterial contamination of the urethra. Recommendations include:
Treatment
A UTI is usually treated with a course of antibiotics. The type, concentration, and length of drug therapy will depend on:
If an infection is due to a sexually transmitted disease, such as chlamydia or gonorrhoea, the doctor will prescribe specific drugs that have been proven to be effective against these organisms. If a person is sexually active and experiencing recurrent UTIs, it may be due to an asymptomatic infection in his or her partner. In some cases, both partners will need to be treated. If a woman is on oral contraceptives, she may want to talk to her doctor as some antimicrobials can lessen their effectiveness.
If a woman is on antimicrobial therapy for several days, there is a chance that she may develop diarrhea or a vaginal yeast infection. This is because the drugs also kill good/normal bacteria and upset the balance of bacteria in the body. If this happens, additional treatment may be required.
Sometimes recurrent or chronic UTIs will occur until an underlying structural abnormality, stone, obstruction, or disease or condition is addressed. For some conditions, surgery may be required to correct the underlying problem
What is Pathology Tests Explained?
Pathology Tests Explained (PTEx) is a not-for profit group managed by a consortium of Australasian medical and scientific organisations.
With up-to-date, evidence-based information about pathology tests it is a leading trusted source for consumers.
Information is prepared and reviewed by practising pathologists and scientists and is entirely free of any commercial influence.
.png)
.png)
.png)
.png)