
This test measures the amount of parathyroid hormone (PTH) in the blood. PTH is released by the parathyroid glands to regulate calcium levels in the body. If PTH secretion is excessive - hyperparathyroidism - it can lead to high levels of calcium or hypercalcaemia. If PTH secretion is too low then low levels of calcium or hypocalcamia can occur. As well as the PTH test being used to diagnose these conditions it can also be used to monitor calcium metabolism in renal failure.
What is being tested?
Parathyroid hormone (PTH) helps the body maintain stable levels of calcium in the blood. It is part of a ‘feedback loop’ that includes calcium, PTH, vitamin D and also phosphate and magnesium. Conditions and diseases that disrupt this feedback loop can cause inappropriate elevations or decreases in calcium and PTH levels and lead to symptoms of hypercalcaemia (raised blood levels of calcium) or hypocalcaemia (low blood levels of calcium).
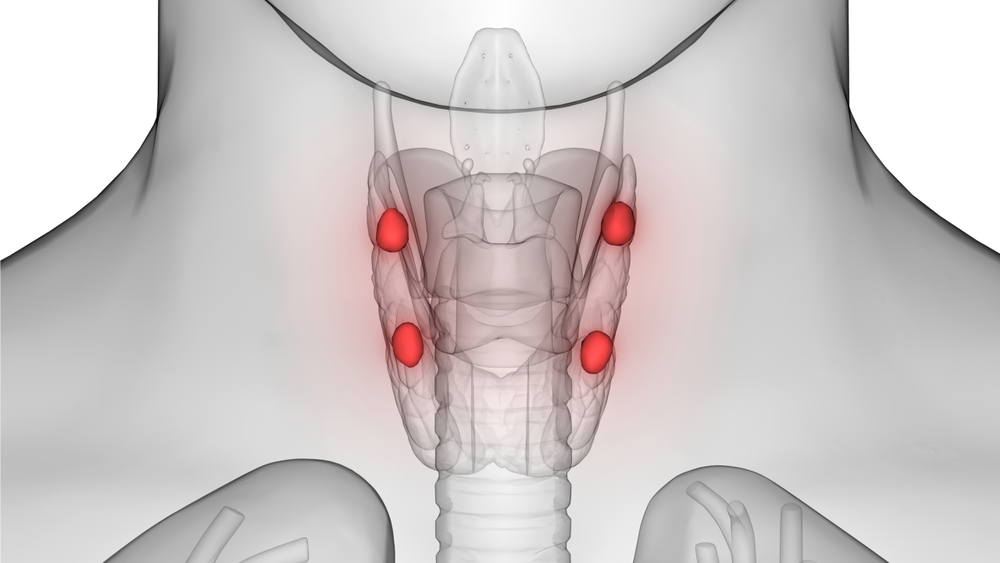
PTH is produced by four parathyroid glands that are located in the neck behind the thyroid gland. Normally, these glands secrete PTH into the bloodstream in response to low blood calcium levels. Parathyroid hormone then works in three ways to help raise blood calcium levels back to normal. It takes calcium from the body’s bone, stimulates the activation of vitamin D in the kidney (which in turn increases the absorption of calcium from the intestines), and suppresses the excretion of calcium in the urine (while encouraging excretion of phosphate). As calcium levels begin to increase in the blood, PTH normally decreases.
Parathyroid hormone itself is composed of 84 amino acids (sometimes called PTH (1-84)). Once it is released from the parathyroid gland into the blood stream, it has a very short life-span; levels fall by half in less than 5 minutes. The fall is caused primarily by the breakdown of PTH to smaller fragments, mainly PTH (35-84) and PTH (7-84). Although it was originally thought that these fragments are inactive, they are, in fact, active but have different actions from PTH (1-84). These fragments, (especially PTH (7-84), seem to do the opposite of PTH: they lower blood calcium levels and prevent removal of calcium from the bone.
How is it used?
PTH is requested to help diagnose the reason for a low or high calcium level, to help distinguish between parathyroid-related and non-parathyroid-related causes. It may also be ordered to monitor the effectiveness of treatment when a patient has a parathyroid-related condition. PTH is ordered along with calcium. It is not just the levels in the blood that are important, but the balance between them and the response of the parathyroid glands to changing levels of calcium. Usually doctors are concerned about either severe imbalance in calcium regulation that may require medical intervention, or in persistent imbalances that indicate an underlying problem.
High blood calcium levels, called hypercalcaemia, may be due to hyperparathyroidism, a group of conditions characterised by an overproduction of PTH by the parathyroid gland. Hyperparathyroidism is separated into primary and secondary hyperparathyroidism.
Primary hyperparathyroidism is most frequently due to a parathyroid tumour (usually benign), that secretes PTH without feedback control. This puts PTH constantly in the ‘ON’ position, where it can cause hypercalcaemia, and can lead to kidney stones, calcium deposits in organs and decalcification of bone. With primary hyperparathyroidism, patients will generally have high calcium and high PTH levels, while phosphate levels are often low.
Secondary hyperparathyroidism is usually due to kidney failure. In patients with kidney disease and/or failure, phosphate may not be excreted efficiently, disrupting its balance with calcium. Kidney disease may also make the patient unable to produce the active form of vitamin D and this in turn means that they are unable to absorb calcium properly from the diet. As phosphate levels build up and calcium levels fall, PTH is secreted.
Secondary hyperparathyroidism can also be caused by any other condition that causes low calcium, such as malabsorption of calcium due to intestinal disease and vitamin D deficiency. With secondary hyperparathyroidism, patients will generally have high PTH levels and low or normal calcium levels. Sometimes, patients with secondary hyperparathyroidism develop a high blood calcium and still have high PTH levels; this is sometimes called tertiary hyperparathyroidism.
Low blood calcium levels, called hypocalcaemia, may be due to hypoparathyroidism, where there is a failure of the parathyroid gland to produce PTH. Magnesium is required for correct functioning of PTH, so low magnesium can be associated with hypocalcaemia. Hypoparathyroidism may be due to a variety of conditions and may be persistent, progressive, or transient. Causes include an autoimmune disorder, parathyroid damage or removal during thyroid surgery, a genetic condition, and severe illnesses. Affected patients will generally have low PTH levels and low calcium levels and will also have high phosphate levels.
PTH levels can also be used to monitor patients who have conditions or diseases that cause chronic calcium imbalances, and to monitor those who have had surgery or other treatment for parathyroid tumours.
Calcium should be monitored at the same time as PTH: it is not just the levels in the blood that are important, but the balance between the two, and the response of the parathyroid to changing levels of calcium. Usually doctors are concerned about either severe imbalances in calcium metabolism (that may require medical intervention) or in persistent imbalances (that indicate an underlying problem).
When is it requested?
PTH may be requested when a test for calcium is abnormal. PTH may be requested when you have symptoms associated with hypercalcaemia, such as tiredness (fatigue), nausea, abdominal pain (stomach ache) and thirst. PTH may also be requested when you have symptoms associated with hypocalcaemia, such as abdominal pain, muscle cramps and tingling fingers. Your doctor may request a PTH, along with calcium (and other tests) at intervals when you have been treated for diseases or conditions that affect calcium regulation, such as the removal of a parathyroid tumour or when you have a chronic condition such as kidney disease.
When a person has hyperparathyroidism, the usual treatment is surgery to remove the enlarged gland or glands. About 85-90% of the time in primary hyperparathyroidism, only one abnormal parathyroid gland is present, but in the remaining cases two or more of the glands is abnormal. In secondary hyperparathyroidism, usually all four of the parathyroid glands are affected. During surgery, it is important for the surgeon to make sure that they have removed all of the abnormal glands. If all are abnormal, this usually means removing three glands completely and part of the fourth, leaving behind just enough parathyroid tissue to prevent hypoparathyroidism. One way to be sure that all of the abnormal tissue has been removed is to measure PTH before and after an apparently abnormal gland has been removed. If all the abnormal tissue is gone, PTH levels will fall by over 50% within 10 minutes. To be useful, this requires that the laboratory be able to provide the results quickly (this is often called rapid or intraoperative PTH measurement).
What does the result mean?
Your doctor will determine whether calcium and PTH concentrations are in balance as they should be. If both PTH and calcium levels are normal, then it is likely that the body’s calcium regulation system is functioning properly.
Low levels of PTH may be due to conditions causing hypercalcaemia or to an abnormality in PTH production causing hypoparathyroidism. Excess PTH secretion may be due to hyperparathyroidism which is most frequently caused by a benign parathyroid tumour.
Calcium - PTH relationship
| PTH | Interpretation |
Normal | Normal | Calcium regulation system functioning OK |
Low | High | PTH is responding correctly: may run other tests to check hypocalcaemia |
Low | Normal/Low | PTH not responding correctly: probably have hypoparathyroidism |
High | High | Parathyroid gland producing too much PTH: may do imaging studies to check for hyperparathyroidism |
High | Low | PTH is responding correctly: may run other tests to check for non-parathyroid-related reasons for elevated calcium |
If calcium levels are high and PTH levels are low, then the parathyroid glands are responding properly, but a healthcare practitioner is likely to perform further investigations to check for non-parathyroid-related reasons for the elevated calcium, such as rare mutations in calcium receptors or tumours that secrete a peptide that has PTH-like activity and increases calcium concentration, which in turn decreases PTH.
Is there anything else I should know?
'Intact’ PTH is broken down by the body (metabolised) into several molecular fragments and tests for PTH may measure one or more of these fragments. None of the assays for intact PTH measure PTH (35-84), which is actually the fragment of PTH present in highest amounts in blood. Many intact PTH assays measure PTH (7-84) as well. In most people, this fragment is present in much lower amounts than PTH (1-84), so this is not a concern.
In kidney failure, a common setting for measuring PTH levels, PTH (7-84) levels increase compared to PTH (1-84), and sometimes over half of what is measured as PTH represents this fragment. Some PTH assays (often called ‘biointact’ or ‘PTH (1-84)’ tests) do not measure this fragment. There is no clear evidence at present that tests that do not measure PTH (7-84) fragments actually are more helpful in kidney failure patients than tests that measure both PTH (1-84) and PTH (7-84), however, results are always lower with the tests that measure only PTH (1-84).
PTH levels will vary during the day, peaking at about 2 am. Specimens are usually taken at about 8 am and are generally collected with a fasting serum calcium level.
Drugs that may increase PTH levels include: phosphates, anticonvulsants, steroids, isoniazid, lithium, and rifampin.
Drugs that may decrease PTH include cimetidine and propranolol.
Common questions
Yes, if your calcium level changes slowly you may not have any noticeable symptoms. In this case, the imbalance will most likely be detected by finding an abnormal calcium level during a regular health check, then by checking your PTH level.
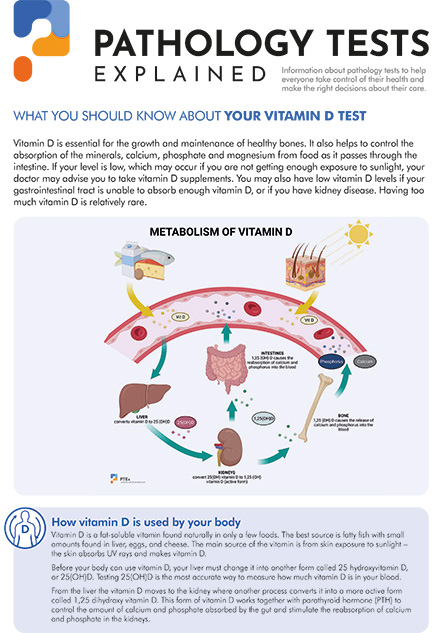
If you do not have enough vitamin D, your body will not be able to absorb calcium properly. Vitamin D regulates the intestinal absorption of calcium, while PTH regulates the activation of vitamin D. Too much and too little vitamin D can cause calcium metabolism imbalances.
Pathology Tests Explained (PTEx) is a not-for profit group managed by a consortium of Australasian medical and scientific organisations.
With up-to-date, evidence-based information about pathology tests it is a leading trusted source for consumers.
Information is prepared and reviewed by practising pathologists and scientists and is entirely free of any commercial influence.
.png)
.png)

.png)
.png)