What is being tested?
This test measures the amount of immunoglobulins A, G, and M in the blood and, in certain circumstances, in cerebrospinal fluid (CSF) . There are numerous conditions and diseases that can cause increased or decreased production of immunoglobulins (Igs).
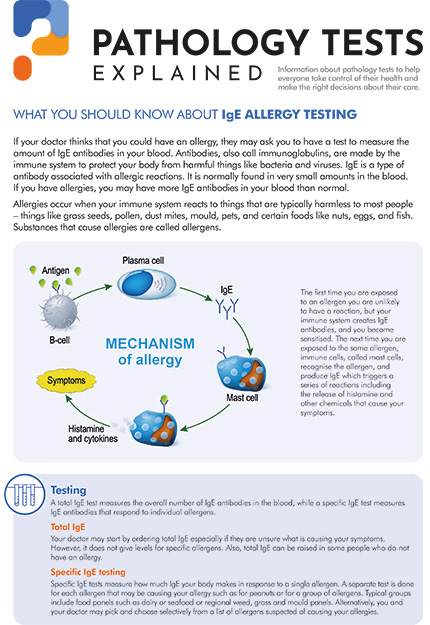
Immunoglobulins play a key role in the body's immune system. They are proteins produced by specific immune cells (plasma cells and B-cells) in response to bacteria, viruses, and other microorganisms as well as substances that are recognized as "non-self" and harmful antigens. The first time a person is infected or otherwise exposed to a foreign substance (antigen), their immune system recognises the microorganism or substance as "non-self" and stimulates cells to produce specific immunoglobulin(s) or antibodies that can bind to and neutralise the threat. With subsequent exposures, the immune system "remembers" the antigen that was encountered, which allows for the rapid production of more antibodies and helps prevent re-infection.
There are five classes of immunoglobulins and several subclasses. Each class represents a group of antibodies and has a slightly different role. Classes of immunoglobulins include:
Quantitative immunoglobulin tests measure the total amount of each primary immunoglobulin class, IgA, IgM, and IgG, without distinguishing between subclasses. Separate testing can be performed to measure immunoglobulin subclasses and/or to detect and measure specific antibodies.
A variety of conditions can cause an increase (hypergammaglobulinaemia) or decrease (hypogammaglobulinaemia) in the production of immunoglobulins. Some cause an excess or deficiency of all classes of Igs while others affect only one class. Some of the conditions are passed from one generation to the next (inherited) and others are acquired.
How is it used?
A quantitative immunoglobulins (Igs) test is used to detect abnormal levels of the three major classes of Igs (IgG, IgA, and IgM) in blood and sometimes in cerebrospinal fluid (CSF) or saliva. It is used to help diagnose various conditions and diseases that affect the levels of one or more of these Ig classes. Some conditions cause excess levels while others cause deficiencies; still others cause a combination of increased and decreased levels.
In general, immunoglobulin disorders can be classified as:
Immunoglobulin excess
Immunoglobulin deficiency
Sometimes an IgM level is used to detect an infection acquired by a newborn before birth (congenital).
When is it requested?
A quantitative immunoglobulins blood test is ordered when a person has symptoms of an immunoglobulin deficiency such as recurrent infections, especially of the respiratory tract (sinus, lungs, and ears) or gastrointestinal tract, and/or chronic diarrhoea.
Immunoglobulins may also be ordered when a person has signs of chronic inflammation or chronic infection and when a doctor suspects excess or abnormal immunoglobulin production. The test may be ordered periodically to monitor the course of a person's condition. An infant may sometimes be tested when a doctor suspects that an infection occurred during pregnancy.
This test may also be performed on cerebrospinal fluid (CSF) whenever a doctor suspects that a condition affecting the central nervous system may be associated with excess immunoglobulin production.
What does the result mean?
The results of the tests for IgG, IgA, and IgM levels are usually evaluated together. Abnormal test results typically indicate that there is something affecting the immune system and suggest the need for further testing. This test is not specifically diagnostic but can be a strong indicator of a disease or condition. There are a number of conditions that are associated with increased and decreased immunoglobulins.
High levels
Increased polyclonal immunoglobulins may be seen with cirrhosis, infections, inflammatory disorders, and some tumours. Monoclonal immunoglobulins are seen in haematologic tumours that involve lymphocytes or plasma cells: lymphoma, Waldenström's macroglobulinaemia, chronic lymphocytic leukaemia and multiple myeloma. In these disorders, there is typically a marked increase in one class of immunoglobulin and a decrease in the other two classes. Although patients may have an increase in total immunoglobulins, they are actually immunocompromised because most of the immunolglobulin is abnormal and does not contribute to the immune response.
The following table shows some examples of conditions that may cause increased immunoglobulins:
| IMMUNOGLOBULIN RESULT | ASSOCIATED CONDITIONS |
| Polyclonal increase in any or all of the three classes (IgG, IgA and/or IgM) |
|
| Monoclonal increase in one class with or without decrease in other two classes |
|
Low levels
Acquired deficiencies, those that are the result of some underlying condition (secondary), may be seen with diseases that cause a general loss of protein, with cancers such as lymphoma, and with severe burns. Deficiencies may also be due to drugs such as immunosuppressants, corticosteroids, phenytoin, and carbamazepine or due to toxins. Inherited deficiencies are rare and may affect the production of all immunoglobulins, a single class, or one or more subclasses.
The most common causes of decreased immunoglobulins are secondary conditions that either affect the body's ability to produce immunoglobulins or increase the loss of protein from the body. The table below lists some of these common causes:
| Conditions/factors that affect immunoglobulin production |
|
| Conditions that cause an abnormal loss of protein |
|
In CSF, immunoglobulins normally are present in very low concentrations. Increases may be seen, for example, with central nervous system infections and inflammatory conditions.
Is there anything else I should know?
Inherited immune deficiencies are rare and are often referred to as primary immunodeficiencies. (For more on this, see the links under the Related information tab). Some of these disorders include agammaglobulinaemia, common variable immunodeficiency (CVID), x-linked agammaglobulinaemia, ataxia telangiectasia, Wiskott-Aldrich syndrome, hyper-IgM syndrome, and severe combined immunodeficiency (SCID).
Infants with otherwise normal immune systems may have temporarily decreased IgG levels when production is delayed. Protection from infections is lost as concentrations of the mother's IgG in the baby's blood decrease over several months. The level of IgG remains at low concentrations until the baby's IgM and IgG production ramps up. This creates a period of time during which the baby is at an increased risk for recurrent infections.
Infants who are breast-fed acquire IgA from breast milk. The IgA in breast milk can be protective against infections, particularly in the time between the decrease of mother's antibodies and the production of the baby's own antibodies.
Those with conditions that cause decreased immunoglobulin levels often do not have a strong immune response to vaccinations; they may not produce a sufficient level of antibody to ensure protection and may not be able to receive live vaccines, such as those for polio or measles.
Many laboratory tests measure antibodies in the blood. Those with immunoglobulin deficiencies may have false-negative results on these types of tests. For example, one test for coeliac disease detects the IgA type of anti-tissue transglutaminase antibody (anti-tTG). If a person has a deficiency in IgA, then results of this test may be negative when the person, in fact, has celiac disease. If this is suspected to be the case, then a quantitative test for IgA may be performed.
Rarely those with IgA deficiency may develop anti-IgA antibodies. When those with anti-IgA are given blood component transfusions that contain IgA (such as plasma or immunoglobulin treatments), they may experience a severe anaphylactic transfusion reaction.
Common questions
A quantitative immunoglobulins test is not considered a routine or a general screening test. It is typically only ordered if your doctor suspects that you have an immunoglobulin deficiency or excess amount. Most people will never need to have one done.
In most cases, immunoglobulins do not respond to lifestyle changes. If you are taking a drug that is decreasing one or more of your immunoglobulins, then you and your doctor may decide to alter your medications. It is very important, however, NOT to discontinue or change your medication dosage without consulting with your physician. Increased amounts may be temporarily reduced by plasmapheresis if medically indicated.
Infants gradually lose protection from infections as the levels of IgG they receive through the placenta from their mothers decrease after birth. Greater protection can be provided for babies through breast-feeding since breast milk contains IgA, which protects against infections. In the first two years of life, the baby’s ability to produce their own immunoglobulin matures.
Not specific ones. Unexplained recurrent infections, multiple infections, or opportunistic infections, with or without chronic diarrhoea, may indicate a need to check a person's immune status. A positive family history of an immunodeficiency may also require follow up. A thorough physical examination and a careful medical history can be critical to a diagnosis.
More information
What is Pathology Tests Explained?
Pathology Tests Explained (PTEx) is a not-for profit group managed by a consortium of Australasian medical and scientific organisations.
With up-to-date, evidence-based information about pathology tests it is a leading trusted source for consumers.
Information is prepared and reviewed by practising pathologists and scientists and is entirely free of any commercial influence.
.png)
.png)
.png)
.png)