

What is it?
Bowel cancer is the uncontrolled growth of abnormal cells within the layers of the tissue that line the small or large bowel. The small bowel is also known as the small intestine and the large bowel is also referred to as the large intestine.
The bowel forms part of the digestive system. The digestive system, or alimentary canal, is the path that food follows through your body. Leaving the mouth, food enters the oesophagus and travels down to the stomach. The food in the stomach empties into the small intestine, or small bowel, and the food passes then to the large intestine, or large bowel. The large bowel is divided into two parts: the colon and the rectum. The colon makes up most of the 1.5 metre length of the large bowel. The colon is responsible for absorbing water, vitamins and minerals from the intestinal contents and conserving them. The rectum is the last part of the bowel, and its function is to form stools, and rid the body of undigested material.

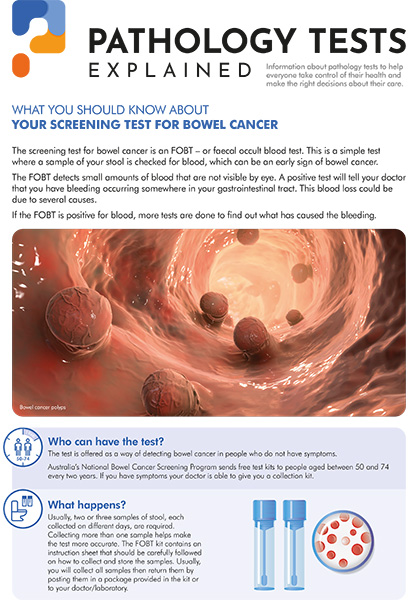
Cancers of the small bowel are very rare. Cancers of the colon are much more common and so are sometimes referred to together as ‘bowel cancer’. Bowel cancer is the second most common cancer in Australia after skin cancer. Each year, there are over 7000 new cases of bowel cancer in men and over 6000 cases in women. Most cases of bowel cancer begin with the development of benign ( or noncancerous) polyps. Polyps are finger-like growths from the wall of the intestine that protrude into the intestinal cavity and are relatively common in people over age 50. Polyps can develop to become cancerous though, and the cancer may invade the normal bowel and spread to other parts of the body (metastasise). These tumours can create blockages in the intestine, preventing elimination of faeces.
The exact causes of bowel cancer are not known, but risk appears to be associated with genetic, dietary and lifestyle factors. Those with a personal or family history of bowel cancer or polyps are at a higher risk, as are those with ulcerative colitis, inflammatory bowel disease and immunodeficiency disorders. A very rare inherited disease, called familial adenomatosis or polyposis, causes benign polyps to develop early in life and cancer develops in almost all affected persons unless the colon is removed. Risk increases with age and with the occurrence of cancers in other parts of the body. High fat and meat diets are risk factors, especially when combined with minimal fruit, vegetable and fibre intake. Lifestyle risk factors include cigarette smoking, obesity and a sedentary lifestyle.
Signs and symptoms
Bowel cancer frequently develops without early symptoms. Symptoms that can occur include:
These symptoms can be caused by cancer or by a number of other conditions. It is important to talk to your doctor and to screen for the presence of bowel cancer. If the polyps that lead to the cancer are detected and removed, bowel cancer can often be prevented. If bowel cancer is detected early, it is up to 90% curable.
Tests
There are many tests useful for screening, diagnosing and monitoring bowel cancer:
Other blood tests may be used to detect the recurrence of treated bowel cancer, such as carcinoembryonic antigen (CEA), or liver function tests to help determine whether there is spread to the liver.
A healthcare practioner, for example a doctor, may perform a digital rectal examination (DRE) with a gloved finger to assess for a rectal mass.
There is also a potential future screening test still in development that looks for mutations in a specific gene (APC gene) that can be detected by analysing the DNA from patients' stool samples.
Treatment
If a doctor finds bowel cancer on biopsy, she or he will want to learn the stage (or extent) of disease. Treatment will depend in part on the stage of the bowel cancer, that is, how far it has spread from its original site.
Staging systems for bowel cancer and the terms used by them vary in different parts of the world, and the most widely accepted systems of staging rely on the extent of spread. In Australia, the staging system for bowel cancer is the Australian Clinico-Pathological Staging (ACPS) System also known as Duke's System.
Stage A – the cancer is confined to the bowel wall
Stage B – the cancer has spread to the outer surface of the bowel wall
Stage C – the cancer is found in lymph nodes near the bowel
Stage D – the cancer is found at distant sites, for example the liver or lungs.
Another commonly used staging system is TNM (Tumour Nodes Metastasis). This system defines the extent of Tumour invasion (T1 to T4), number of local lymph Nodes affected by the tumour (N0 to N2), and whether the tumour has spread to a distant site or not (termed Metastasis – M0 or M1).
Further details on staging can be found on the Bowel Cancer Australia web site.
All stages of bowel cancer are usually treated by surgically removing the cancer and possibly some of the surrounding tissue. For Stages B and C, chemotherapy and/or radiation therapy may be added to help kill the cancer and shrink the tumour. Chemotherapy and radiation may also be used in Stage D to improve symptoms and to prolong life.
Targeted therapy is a relatively new approach to treatment that uses drugs to target specific proteins that control cell growth and maturation. Malfunctioning proteins may contribute to a cancer's uncontrolled growth. For example, drugs such as cetuximab attack the epidermal growth factor receptor (EGFR). Targets therapies such as these may have less severe side effects than standard chemotherapy.
Immunotherapy is also relatively new and may be used to treat some patients with colon cancer. Immunotherapy works by helping a patient's own immune system recognise and kill cancer cells more effectively.
Pathology Tests Explained (PTEx) is a not-for profit group managed by a consortium of Australasian medical and scientific organisations.
With up-to-date, evidence-based information about pathology tests it is a leading trusted source for consumers.
Information is prepared and reviewed by practising pathologists and scientists and is entirely free of any commercial influence.
.png)
.png)

.png)
.png)