
What is being tested?
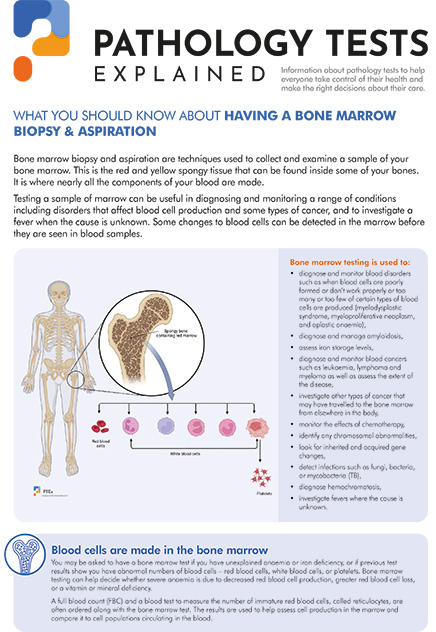
Bone marrow is the production site of the blood cells. It contains the precursors of red blood cells, platelets and white blood cells.
Bone marrow aspirate allows the pathologist to examine (under the microscope) the types, numbers and the appearance of blood cells. Additional tests might include:
How is it used?
The bone marrow biopsy and aspiration provide information about blood cell production. They are not routinely ordered and in fact the majority of people will never have one done. A marrow aspiration and/or biopsy may be ordered to help evaluate blood cell production, to help diagnose leukaemia, to help diagnose a bone marrow disorder, to help diagnose and stage a variety of other types of cancer (to determine spread into the marrow), and to help determine whether a severe anaemia is due to decreased red blood cell (RBC) production, increased loss, abnormal RBC production and/or to a vitamin or mineral deficiency or excess.
A bone marrow sample may also be evaluated and cultured for the presence of microorganisms such as fungi, bacteria, or mycobacteria (such as that which causes tuberculosis) when the patient has a fever of unknown origin. Bone marrow testing may be ordered when it is suspected that the patient has a chromosomal abnormality and/or a disorder associated with iron storage that may cause iron to accumulate in the marrow.
When a person is being treated for a cancer, a bone marrow aspiration and/or biopsy may be ordered to evaluate the response to therapy to determine whether suppressed marrow function is beginning to return to normal.
A full blood count (FBC) and reticulocyte count are frequently ordered along with the bone marrow aspiration/biopsy. The results are used to help evaluate cell production in the marrow and compare it to current cell populations in circulation.
When is it requested?
Your doctor may order this test if you have abnormal result on a full blood count (FBC) or complete blood count (CBC). This could include abnormal numbers or types of red blood cells, white blood cells or platelets.
Various disorders could be diagnosed on bone marrow aspiration and/or biopsy:
It is also performed to monitor the treatment efficacy or if relapse is suspected.
What does the result mean?
With a bone marrow biopsy and aspiration the doctor is evaluating what is in the marrow in order to determine whether the cells found are normal and present in typical quantities, to determine whether there are cells present that shouldn't be there (such as abnormal cells that are characteristic of specific cancers or disorders such as the Gaucher cell found with Gaucher's disease or the foamy lipid-filled Niemann-Pick cell found with Niemann-Pick disease), and to determine what is missing.
The training and expertise of the pathologist or haematologist evaluating the marrow samples allows them to sort through the marrow clues and tell the doctor what is happening in the marrow. In most cases, this information can confirm or rule out a diagnosis and bone marrow involvement, but it can also point out the need for further investigation. For instance, if there are a decreased number of RBCs in the blood and an increased number of reticulocytes, and a marrow evaluation shows that RBC production appears normal but increased, then the doctor knows that marrow production of RBCs has increased appropriately to meet a RBC demand. What they still do not know is the reason for the demand. It could be due to an acute or chronic loss of RBCs (such as may occur with gastrointestinal bleeding) or due to acute or chronic RBC destruction (such as sometimes occurs with an artificial heart valve).
A patient with few RBCs and no increase in reticulocytes may have aplastic anaemia (suppressed RBC production in the marrow). An evaluation of the bone marrow may confirm this condition but it does not necessarily tell the doctor whether it is due to a bone marrow disorder, radiation, exposure to certain chemicals, some cancers, cancer treatment or due to a tuberculosis infection.
The doctor takes the information that they receive from the marrow evaluation and combines it with information from a clinical examination, blood tests and a variety of other tests, such as imaging scans and X-rays, to reach a final diagnosis. It can be a straightforward process or it can be a complex diagnostic puzzle. Patients should stay involved in this process by talking to their doctor before and after a bone marrow biopsy and/or aspiration, asking what their suspicions are, what kind of information they are hoping to obtain from the evaluation, and what follow-up tests might be indicated.
Common questions
It is not usually necessary, but you may be given a sedative before the procedure.
The collection process is similar but the bone marrow donor goes through a physical examination and has blood tests done prior to the collection to make sure that they are healthy and that their sample will be compatible with the person to whom the marrow will be donated. The donor is usually put under general anaesthesia during the collection because a larger amount of marrow must be obtained under sterile conditions. The sample is then processed, filtered and given to the transplant recipient through a vein.
Pathology Tests Explained (PTEx) is a not-for profit group managed by a consortium of Australasian medical and scientific organisations.
With up-to-date, evidence-based information about pathology tests it is a leading trusted source for consumers.
Information is prepared and reviewed by practising pathologists and scientists and is entirely free of any commercial influence.
.png)
.png)

.png)
.png)

